HIV/AIDS, Population and Sustainable Development
Victor Angelo
p. 99-120
Abstracts
The wide-ranging impact of HIV/AIDS on demographic trends and socio-economic development of African countries deserves renewed attention and additional research. HIV/AIDS severely undermines the development prospects of many African countries, most of which have recorded shockingly high prevalence rates of the epidemic. In the years to come, Sub-Saharan Africa is far more certain to experience further demographic changes that would continue to impact negatively on development trends. The epidemic is decimating human capital and institutions, perpetuating intergenerational poverty and inequality, and threatening the security of populations and countries. In this regard, it has become one of the most serious challenges facing African countries. This paper asserts that in high HIV prevalence countries, the majority of which are in Sub-Saharan Africa, the size, composition, structure and distribution of populations have experienced profound mutations. The new demographic structure has a direct and significant bearing on all facets of sustainable development. It is therefore essential to examine how these demographic modifications affect efforts towards socio-economic progress.
Outline
Full text
1. Introduction
1The wide-ranging impact of HIV/AIDS on demography trends and socio-economic development of African countries deserves renewed attention and additional research. HIV/AIDS severely undermines the development prospects of many African countries, most of which have recorded shockingly high prevalence rates of the epidemic. Against the background of alarming data on the prevalence of HIV/AIDS in some countries in Sub-Saharan Africa, epidemics and dynamics of the pandemic have moved beyond the confines of public health issues to serious demographie and sustainable development concerns. African governments, the international community and non-governmental organizations have recognized the great magnitude of HIV/AIDS in Africa and its far-reaching implications worldwide. This recognition has led to the adoption of various national, regional and global initiatives in response to the epidemic.
2This paper is premised from the standpoint that notwithstanding the various initiatives to combat HIV/AIDS, the epidemic remains a serious setback to development. The paper asserts that in high HIV prevalence countries, the majority of which are in Sub-Saharan Africa, the size, composition, structure and distribution of populations have experienced profound mutations. The new demography structure has a direct and significant bearing on all facets of sustainable development. It is therefore essential to examine how these demography modifications affect efforts towards socio-economic progress. To achieve this objective, the paper seeks to explore some of the emerging issues that are relevant to the analysis of the interplay between HIV/AIDS and the impact of the ensuing negative demography trends on various aspects of sustainable development. Attention will also be directed at the important, but relatively overlooked dimension of human security in the discourse of HIV/AIDS.
3The focus of this paper is Sub-Saharan Africa, a region where development is most compromised by the HIV/AIDS epidemic. The soaring prevalence rates of HIV make the region to stand out as the present epicenter of an increasing global pandemic. The effects of HIV/AIDS on the region cut across all sectors and aspects of life. The disease is decimating human capital and institutions, perpetuating intergenerational poverty and inequality, and threatening the security of populations and countries. It has become one of the most serious challenges facing African countries.
4The first part of the paper will therefore examine the magnitude of the HIV/AIDS epidemic in Sub-Saharan Africa by making comparisons with other regions of the world, based on estimates and projections from various sources, especially the United Nations. The objective is to illustrate the extent to which the pandemic has become a dominant development challenge to many Africa countries. Though some of the data may portray dramatic scenarios based on projections, they serve to underscore the rapid spread of the HIV infection, the challenges facing African countries as well as the need for strong commitment to scale up responses to stem the epidemic. The second part will look at how HIV/AIDS modifies demographic factors and the implications of these changes. The interplay between the high prevalence of the epidemic and demographic factors such as life expectancy, mortality, fertility and growth rates will be considered in the analysis. The epidemic is taken as a significant determinant of the size, composition and structure of national, regional and global populations. The third section looks at how population trends influenced by HIV/AIDS directly impact on sustainable development in the affected countries. It seeks to show that HIV/AIDS has become a destructive force requiring action that goes beyond treating the epidemic as a health crisis. It has become a serious threat to socio-economic development and the stability of countries. The last part of the paper will consider the various on-going efforts, notably by the UN, to stem the growing challenges of HIV/AIDS.
2. Magnitude of the HIV/AIDS problem in Africa
5HIV/AIDS has presented enormous shocks to international development It is considered the world's fourth biggest killer and Africa's leading cause of death. UNAIDS estimates that over 60 million people throughout the world have been infected by the HIV virus since the epidemic began two decades ago. The alarming data presents a bleak future, particularly in the least developed countries, where the magnitude of the epidemic is great.
6In Sub-Saharan Africa, a region carrying a disproportionately large population of infected people, over 28 million people are infected (TABLE 1). The rapid spread of the pandemic is not confined to Sub-Saharan Africa, but is also affecting countries in other regions. In countries such as India and China, approximately 4 million and 1 million people, respectively, are living with HIV1. While HIV/AIDS is spreading rapidly in Eastern Europe and Central Asia, the number of infected people in all regions is still low compared to Africa. Australia and New Zealand carry the lowest figure.

7Taking into consideration the large populations of most of the developed countries, notably in Western Europe and North America, the number of infected people is relatively low. The high levels of socio-economic development in these countries, providing the prerequisites for appropriate and timely interventions in terms of prevention and effective health education, could be primarily attributed to this fact. These conditions are absent in most of Sub-Saharan Africa.
8Among the number of people killed by AIDS in 2001 an estimated 580 000 were children under the age of 15, and almost 90% were Africans2. The implications of HIV/AIDS in Africa are not limited to infection, but also to affecting their entire lives as children. The majority of adults infected by the HIV virus or dying of AIDS are parents of young children. In some cases the children they leave behind were infected at birth or during breast-feeding.
9The number of children who have lost one or both parents to HIV-related illnesses in Africa is approximated at 11 million, and it is projected to rise to 20 million by 2010, resulting in the emergence of more vulnerable youths joining the already huge population of unemployed youths3. In the same distressing light, UNFPA established that half of all new infections are among the age group of 15 to 24 years. In its 2003 report, Making One Billion Count: Investing in Adolescence Health and Rights, UNFPA gives an alarming picture for the future. It estimated that a youth is infected with HIV every 14 seconds, with increasingly females accounting for nearly half of HIV infection worldwide, due to biology, gender and cultural norms.
10A similar pattern in global estimates is followed in terms of the regional distribution of the total number of young people living with HIV/AIDS. Sub-Saharan Africa, with over 8 000000 young people infected, carries the largest population of infected youths in the world (TABLE 2). An estimated two-thirds of newly infected youths aged 15 to 24 years in the region are female. The large percentage of infected females, which even surpasses the global average of 62%, is cause for great concern as it implies a tragic legacy for African countries already struggling to sustain decades of progress made in raising life expectancy and gender equality.

11The average prevalence rate for Sub-Saharan Africa estimated at 9% is exceptionally high compared to the estimated global average of 1.2%, demonstrating the magnitude of the pandemic in the region (TABLE 3). The average sub-regional rate though does not portray the accurate situation as the range in the variance of rates is large. The cross section of selected countries represents different levels of prevalence from extremely and moderately high rates to relatively low rates. The huge disparities in the prevalence of the HIV virus in various countries could be attributed to the varied levels of awareness of the populations. Some countries are strongly committed to fight the epidemic, hence the great strides in raising awareness. Others have had a slow response to the pandemic, resulting in considerably low levels of awareness among their populations. Low prevalence rates could also be attributed to the timing of countries with respect to their experience with the pandemic. In some countries, the pandemic is a new challenge that has yet to reach its peak while in others, the epidemic has peaked to the levels of an emergency. There are countries that adopted effective national responses. Uganda has been singled out for successfully subduing a major epidemic by reducing the prevalence rate from 8.3% in 1999 to 5.0% in 20014. The early adoption of a multi-sectoral response has been ascribed to this achievement. Senegal has also been hailed as a success story for maintaining the prevalence rate at a low level of 1.43% for a population of 9 200 0005. This has been credited to strong political commitment and social mobilization at all levels of society to fight the pandemic.

12The variation also extends to regions within the continent. Of significant note to this trend are the seven countries in the Southern Africa region showing prevalence rates higher than 20%, rates not reflected by any countries north of that region. The high rates have largely been blamed on the increased mobility of populations across countries within the region and similar risky practices based on cultural norms. The interconnectedness of the economies in the SADC region has intensified the movement of people across countries through immigration and trade. The movement of truck drivers, informal traders and illegal immigrants across borders, particularly from many of the countries to South Africa where economic opportunities are considered greater, is a factor frequently cited for the high incidence of HIV infection in the region.
13The high rates have also been ascribed to cultural practices that place women on a lower social status than men, disadvantaging them economically and ultimately reducing their ability to negotiate safe sex. Though economic hardships have been directly associated with the adoption of risky sexual behaviours, as coping mechanisms, that expose one to HIV infection, the epidemie has spread across social classes and ethnic groups. The reasons cited for the high prevalence of HIV infection in the epidemicion should be advanced with caution as the same factors could apply to all sub-regions on the continent such as West and East Africa. Furthermore, economic hardships are prevalent throughout Africa, albeit in varying levels. It is however true that Southern Africa was submitted to a different colonial process that separated the indigenous workers from their families, for long periods of time, creating therefore additional social conditions for sexual activities to take place outside the family structure. This is an issue that remains largely ignored in the studies about HIV prevalence in the Southern Africa Region.
3. Demographic impact of HIV/AIDS
14The HIV/AIDS epidemic has had considerable and sometimes dramatic impact on mortality rates, life expectancy, and population growth rates. The rapid change in these indicators has modified the key demographic variables in many countries.
15Change in life expectancy at birth, defining the average number of years a newly born is expected to live at current national levels of mortality, is one of the most direct indicators for development. It indicates the progress a country has made in improving the standard of living in terms of factors such as income, health and education, resulting in longer lives for its population. With the advent of immunization, treatments for various diseases, better health delivery systems and relatively improved standards of living, life expectancy had improved considerably in many countries in Africa in the past decades. Current trends show that HIV/AIDS, by killing and incapacitating adults in the prime of their lives, undercuts human security and derails development leading to dramatic decline in life expectancy of affected countries. The high incidence of HIV infection within the age group 15 to 24 years means that the majority die before they reach their thirties. A comparison of life expectancy within the context of the prevalence of HIV/AIDS to the expected life expectancy without AIDS in countries with high prevalence rates clearly illustrates this trend (Figure 1). Due to the prevalence of HIV/AIDS, the populations of the selected countries lose more than two decades of living, with Zimbabwe for instance showing a loss of 35 years. The levels of life expectancy in Africa are being reversed to levels of probably five decades ago, before these countries had made advances in socio-economic development (TABLE 4). In all the cases selected, life expectancy has declined significantly, with Botswana, Lesotho, Swaziland and Zimbabwe most affected.


16The epidemic has had an unprecedented influence on the trend of infant and child mortality. According to UNAIDS 2002 Report on the Global HIV/AIDS Epidemic, almost 500 000 African children died of AIDS related illnesses in 2001. Estimates put the global figure of infected children under 15 years of age at 4 million. Infants acquire the disease from their mothers during pregnancy, delivery or breastfeeding. Between 30 to 40% of babies born to HIV positive mothers are infected and the majority will not survive to age five. Infection among children is being exacerbated by the increasing incidence of child sexual abuse. The progression of the HIV infection to AIDS in children is rapid, meaning that the majority of these children do not reach adulthood as they die early. The selected countries in TABLE 5 show a large increase in under-five mortality in six of the most affected countries, all in Southern Africa. Zimbabwe, for instance, from 1995 to 2000 shows a rate of 124 per 1000 births, already double what would have been without AIDS. Though the rate is expected to decline by half by 2015 to 2020, it will remain around double the level of «Without AIDS».

17The number of children killed by AIDS, added to the number of children dying from other causes, indicate a drastic reversal of decades of progress made by African countries in stemming child and infant mortality. HIV/AIDS has led to unprecedented increase in child and infant mortality erasing achievements made in immunization. As infant mortality increases, life expectancy at birth decreases.
18The rising mortality has significantly slowed population growth and in some cases reduced population size. Substantial decline in reproductive potential due to AIDS mortality also reduces the level of population growth. In Sub-Saharan Africa, among all newly infected people between the ages of 15 to 24 years, 67% are women6. Most of these women die before completing their expected fertility cycles. Fertility rate, representing the number of children born per woman, if all women completed their expected cycles, is negatively affected by the HIV infection. Recent studies indicate that fertility among HIV positive women is substantially lower than among uninfected women due to biological changes resulting from infection. Following such studies, the UN Population Division concluded that the fertility rate of those infected with HIV is 25% to 40% lower than that of those not infected. Furthermore, spontaneous abortions were observed to be more prevalent among women infected by the HIV virus than those who are not7. This is primarily attributed to non-voluntary factors, especially relating to the depressing effect of STIs on fertility. There could however be other closely related factors influencing the decline in fertility. In some instances, strong awareness could encourage change of sexual and contraceptive behaviours. It could also delay the onset of sexual activity, encourage abstinence and also boost the consistent and regular use of condoms.
19African countries have been making efforts to reduce their populations for decades through education, family planning and accessibility to contraceptives. The current decline in population has also been influenced by the dynamics of the HIV/AIDS pandemic that are expected to have dire consequences for some of the most affected populations. Countries recording high HIV prevalence rates indicate marked impact on population size and growth (TABLE 6). While the populations of the affected countries will grow steadily, the rates will be low. Botswana and Lesotho, for instance, by 2020 will have a growth rate 30% lower than would obtain without AIDS. A particularly lower growth rate is projected for South Africa, averaging 0.08% during 2000 to 2020 and being 95% lower than it would have been without AIDS. This trend is attributed to both the high prevalence of HIV/AIDS and the relatively low fertility characterizing the country8.

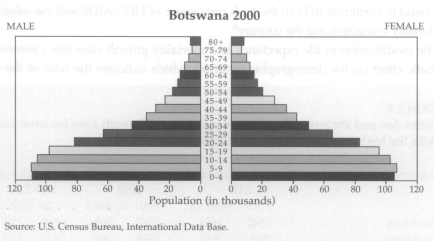
20The modification in life expectancy and mortality growth rates has a somewhat dramatic effect on the demographic pyramid, which indicates the ratio of the economically dependent (0 to 14 and over 65 years) to the economically productive populations (15 to 64 years). The high mortality and lowered fertility that occur in the middle part of the pyramid indicates an increase in the burden placed upon the productive group by the dependents, The epidemic increases the dependence ratio as the working population succumbs to AIDS, leaving the burden of care of households to the elderly, who also require care. The US Bureau of Census described the evolution of such a pyramid in Botswana, as a change from the sex-age pyramid to a «chimney», where the upper sides of the pyramid become vertical (Figure 2). Such an evolution leads to an increase in dependency and reduction in production affecting all sectors including health, education, agriculture and business.

4. HIV/AIDS and sustainable development
21The modified demographics have a direct bearing on human and social development in Africa. Given the soaring rates of HIV infection, the goals of sustainable development are increasingly compromised. The high mortality and reduced life expectancy weaken economic, social and political structures, threaten human security and make vulnerable groups, such as women and children, more vulnerable than they were before the epidemic. Human capacities in all sectors are depleted by AIDS related deaths or illness as well as eroded by the related morbidity; institutional capacities are overwhelmed by increased demands for health care; social fabrics are destroyed as family members succumb to AIDS; and vulnerabilities of women and children increase as they grapple with the burden of care, and in the case of children as they are thrust into a life without parental support and guidance.
22To appreciate the scope of the impact of the pandemic on sustainable development, it is necessary to understand the term in general, and within the context of high HIV prevalence. The term has generally been understood within the narrow confines of environmental protection and related areas. However, environmental protection is just one aspect of the many segments of sustaining development. Sustainable development ensures a better quality of life for all human beings now, and in the future. It connotes human development. In this regard, the United Nations World Commission on Environment and Development (the Brundtland Commission), in 1987, coined the now widely used definition of sustainable development. It defined the concept as development, which meets the needs of the present without compromising the ability of future generations to meet their own needs. Goodland and Ledec similarly but elaborately define sustainable development as, «a pattern of social and structural economic transformation (i.e. development) which optimises the economic and other societal benefits available in the present without jeopardising the likely potential for similar benefits in the future»9. Bothdefinitions imply a sustainable process and outcome that seeks to increase the capabilities and opportunities for people to exercise those capabilities.
23UNDP, in its annual Human Development Reports, attempts to move from the preoccupation with economic growth and the creation of wealth to the well being of people in measuring development. It pioneered and popularised the term human development to make people pivotal to sustainable development. UNDP views the basic goal of development as the creation of an environment that enables people to enjoy long, healthy and creative life by expanding their choices, freedom and dignity. The variables used in measuring development in this regard put people at the centre of the process and the goal. These are: life expectancy; adult literacy; education enrolment ratios and gross domestic product per capita. The active participation of the people is indispensable to the process and the outcome of development. The needs of the present are thus met by having a society with healthy people and a growing economy, a properly managed environment, transparency and equitable distribution of resources and participation of people in decisions and actions that benefit them, taking into account the implications for the future. Progress in development is not only sustained from one generation to the next, but it also sustains the existence of people now and in future.
Impact on households
24The most severe impact of HIV/AIDS has been felt at the household level. The illness or death of a member of the household means reduced or loss of household income, declining productivity and enormous loss of household savings due to medical, care and funeral costs. There is also a reallocation of labour as the most economically productive members die, leaving the elderly and young children, less endowed in skills and ability to produce. The impact of HIV/AIDS is usually great on poor households, which are the least prepared to cope with such problems. By its nature, AIDS could kill more than one member of the family, as spouses or partners and children may also be infected, increasing the financial and psychological strain on households. The general well being of surviving members of the households declines due to economic hardships, illness and grief from losing a relative. In some instances, the family unit disintegrates. Surviving members of such households, including children, may be forced into very low paid work, crime or sex work, which would in turn perpetuate the epidemic.
Reduced human and institutional capacities
25While HIV/AIDS affects both the public and private sectors, the immediate impact on development is felt in the health and education sectors. In the public health sector, for instance, the increasing need for medicine and care for people with HIV related illness puts significant strain on resources and structures. In most African countries these facilities are already inadequate due to financial constraints. Increased demand for the facilities drains the meager public resources. The problem of health care facilities is compounded by reduced human capacities as health personnel succumb to AIDS.
26The education sector is equally affected as demand for supply of education is disturbed. Orphans without parental support drop out of school, as they look for means of sustaining themselves or as they become caregivers. Teachers succumb to AIDS, depriving children of education. The pandemic has had a severe impact on education in Sub-Saharan Africa, destroying the already struggling sector.
27In other segments of the public sector, overall mortality in some countries has risen over the past decade largely due to AIDS and will result in governments losing the ability to supply essential goods and services. In addition, institutional memory and skills are also lost with the deaths. The private and informal sectors, which employ significant numbers of people in Africa, are not spared from the impact of HIV/AIDS on human capacity. Agriculture, which is the mainstay of most African economies, is severely affected, threatening food security on the continent.
Economic impact
28The most severe impact of HIV/AIDS on the economy of affected countries relates to the indirect costs from reduced economic growth and activity due to increased mortality and morbidity. These costs arise from absenteeism due to illness and funeral attendance, lost skills, reduced work performance and lower productivity, particularly in labour-intensive businesses. A World Bank study suggests that even an adult prevalence rate of 10 per cent may reduce the growth of national income by up to a third and infection levels above 20 per cent can reduce a country's GDP by 1 per cent per year10.
29The epidemic transforms the characteristics of the labour force in terms of its size, composition, health, education and skills and this has a direct bearing on the performance of any economy. In the worst affected countries, particularly in Southern Africa, it is projected that by 2010 the labour force will be 20% smaller than it should be without AIDS11. All sectors in Sub-Saharan Africa are affected, making it increasingly difficult to replace skilled as well as unskilled labour lost to HIV/AIDS. As HIV infection is largely concentrated in the working age population of 15 to 49 years, the composition of labour force is upset. HIV/AIDS has also led to high labour mobility and migration as individuals escape the economic hardships and deteriorating as well as overburdened social services, to better opportunities. This mobility has in part determined HIV transmission, particularly in Southern Africa where mobility is relatively high.
30Coupled with the low level of savings and reduced investment, the epidemic has dire consequences on the struggling economies of Africa. The economies are also strained by the increasing demand for resources for care, prevention and treatment placed on health and other social services. Demands for training and skills to replenish those lost to AIDS deaths also strain the economy. The failure of the economies to grow increases poverty among the populations of these countries.
31While the direct link between poverty and HIV/AIDS is complex, economic hardships have and continue to expose poor people to HIV infection through risky sexual behaviours such as prostitution and «transactional sex» (exchanging sex for food, tillage and agricultural inputs, jobs or other basic necessities), as coping mechanisms. Consequently, the poor people feel the burden of the epidemic since they cannot afford the treatment and care, and they have to engage in behaviours that increase the risk levels.
Impact on gender relations
32The most dramatic impact of HIV/AIDS on gender relations pertains to the erosion of the huge progress made in gender equality in Africa. Women, due to biological, social, economic and cultural factors, are more vulnerable to HIV infection than men. Young women are even more vulnerable to infection as they have their sexual experiences earlier than young men and in most cases with older men, who are already infected.
33The prevalence of HIV/AIDS has a direct bearing on the perpetuation of inequalities between women and men. Women, particularly young ones and the elderly, are also more affected by the epidemic as they assume the largest burden of caring for those dying of AIDS and the orphans left behind. Young girls drop out of school to take care of sick relatives and orphaned siblings. With no education, these women are doomed to a life of poverty, which exposes and increases their vulnerability to HIV/AIDS. They are not empowered to negotiate safe sex or to refrain from engaging in risky sexual behaviours to sustain themselves. These continuing inequalities play a significant role in the processes of HIV transmission to women.
Impact on youths
34The impact HIV/AIDS on youths has profound implications for the future of African countries at two levels. The first level relates to the growing number of child sexual abuses, a disturbing factor fueling the spread of the virus among young children, both females and males. The Special Rapporteur on the Sale of Children, Child Prostitution and Child Pornography of the UN Commission on Human Rights (UNCHR), found that in South Africa, for instance, reports of young children being targeted as sexual partners in order to reduce the risk of contracting HIV/AIDS were common. The most worrying dimension to the increase in child sexual abuses is that some of the perpetrators are infected by the HIV virus and thus believe that sex with a virgin would cure them. Media reports indicate that this tendency is not confined to South Africa, but also to some of the countries in the region. In some instances, these cases go unreported because the perpetrators are family members or individuals known to the families. Information on such abuses against children in the various African countries is not easily available to make an analysis of the extent of the problem. However, the foregoing report highlights the serious implications on child mortality rates.
35The other level pertains to the increasing challenges presented by the growing number of orphans, overwhelming the existing social support systems. Furthermore, the general economic decline in most African countries has changed societies such that the traditional safety nets of extended families and communities that used to exist for orphans decades ago are almost non-existent at present.
36While AIDS orphans account for a proportion of the total number of children orphaned by other causes in Africa, their increase in numbers has implications for intergenerational poverty and human security in Africa. The death of a parent or both parents at times mean the disintegration of the family unit, forcing young children to fend for themselves. Many of these orphans drop out of school to form child headed households to look after their siblings or live on the streets until they reach adulthood. In cases where orphans are taken into the care of grandparents or relatives, their lives are never the same as these guardians may lack parenting capacities due to old age, lack of resources or lack of care.
37The pandemic has contributed significantly to the increasing number of street children. The trauma of losing parents as well as the lack of economic and educational opportunities and poor socialization could lead to anti-social behaviour such as crime, rebellion and prostitution. These affected children grow up with less economic opportunities and become less productive in society as adults. The greatest threat associated with this trend is the emergence of a «lost generation», most vulnerable to abuse, sex work or emotionally unstable HIV infected generation, particularly females, because of their vulnerability to sexual violence, sex work or emotionally unstable relationships and HIV infection.
5. HIV/AIDS and security
38The pandemic has serious implications for security in Africa as it impacts on all facets of existence of an individual, a community or a state. The understanding of the impact of the epidemic on security has generally been confined to studies on the prevalence of the disease on military and police forces in relation to peacekeeping missions as well as on the spread of the epidemic among communities in conflict areas. Considering the huge threat presented by the increasing number of people made vulnerable by AIDS, particularly orphans, it is essential to broaden the understanding.
39Security within the context of the epidemic should thus include all aspects of human security.
40The 1994 UNDP Human Development Report introduced the now commonly used concept of human security that associates security with people and sustainable development rather than with armaments and states. The Report provides a comprehensive definition of the concept. The first element of the concept of human security relates to the safety of people from such chronic threats as hunger, disease and repression. The second refers to the protection of individuals from sudden and hurtful disruptions on the pattern of daily life — whether in homes, in jobs or in communities. In a related but expanded definition, the final report of the Commission on Human Security (2003) asserts,
«human security is protecting vital freedoms. It means protecting people from critical and pervasive threats and situations, building on their strengths and aspirations. It also means creating systems that give people the building blocks of survival, dignity and livelihood. Human security connects different types of freedoms — freedom from want, freedom from fear and freedom to take action on one's own behalf».
41The central idea of the interlinked elements of human security is the safety of individuals. There is a great emphasis on the people, rather than on territories, which are traditionally associated with the security of the state. However, insecurities of people at any level present threats to the stability of the state as an unstable state impacts on the personal security of its people. The Commission on Human Security further stresses the need for conditions that are conducive to empower people to maximize their potential to make decisions and to freely participate in development.
42HIV/AIDS significantly impacts on critical elements of human security. The pandemic increases the vulnerability of children, thus eroding their personal security. The loss of parental protection exposes children to physical violence in the form of abuses, including sexual abuse. The common incidence of children infected by the HIV virus through sexual abuse is a case in point. The loss of parental protection also enhances risks of psychological imbalances among traumatized children, seriously affecting their relations with society. The children's opportunities to enjoy healthy and productive lives are destroyed. Women are equally affected as the perpetuated gender inequalities leave them economically insecure further exposing them to the HIV infection and limiting their choices and opportunities in health, education and food production. The prevalence of HIV/AIDS in Africa, where inadequate resources limit treatment and care, erodes the protection of vulnerable individuals from opportunistic infections. In addition, once HIV infected individuais become ill, they lose the physical ability to work or access food.
43The impact of the epidemic on state security also provides a crucial dimension to human security. Personnel in the various public service institutions are succumbing to AIDS further weakening the institutions and disrupting service delivery. The impact of the high mortality and morbidity on these institutions has considerable implications for state security as it erodes public confidence in a government. Furthermore, the loss of police, military and judiciary personnel, for instance, has direct effects on the rule of law, effective policing and the defense of the country. Many military forces in Africa are reported to have HIV infection rates as much as five times that of the civilian population12. The resultant situation leaves communities vulnerable to further infections and also to increased crime, civil instability and even threats from attacks outside the national borders.
44Amidst the weakening security institutions, there is a growing population of less educated, unemployed and badly socialized children. There has not been adequate consideration given to the looming threats to both human and state security from such a development. Possible scenarios are necessary to illustrate the gravity of the problem to the security of African countries. The best-case scenario is one that sees national governments adopting as a matter of urgency policies and interventions that address the growing problem of vulnerable children, including AIDS orphans. In this regard, the children are provided the safe conditions to maximize their full potential in life and become productive members of society. The worst-case scenario is based on the perpetuation of the present situation where most orphans are ending up on the streets or heading households without resources and capabilities. The tendency of such traumatized children to become violent and rebellious in their quest to have personal security is not surprising. They carry through these behaviours into adulthood.
45These marginalized youths could be easily lured into activities that promise immediate food and other commodities, or prospects of «family» bonds they so much desire. They could become criminals or join violent gangs. The various internal wars in Africa have often included the participation of child soldiers. With a large number of unproductive youths, this phenomenon could remain a regional challenge for years to come. Orphans could find their alternatives in rebel movements and militias. Possession of a gun by a young boy infected by the HIV virus would give him a sense of power over society. The boy is expecting to have a short life as a result of AIDS and he has nothing to lose by using the gun to sustain himself. This scenario provides a frightening picture for the future. Orphans could easily become mercenaries in future. They threaten all aspects of human security worsening the development and national security problems already in existence.
46The challenges presented by orphans create a vicious cycle of intergenerational poverty as their choices and opportunities as adults remain limited, impacting negatively on sustainable development. In this regard, the interplay between sustainable development and human security entails the former being a process of widening the range of people's choices, and the latter to provide the environment conducive for people to exercise these choices safely and freely, guaranteed that the existing opportunities to do so will be available in future13.
6. Global efforts to combat HIV/AIDS
47It has been widely acknowledged at the national, regional and global levels that the pandemic has grave consequences for development in Africa. National governments, bilateral and multilateral cooperation partners, and non-governmental organizations (NGOs) have formed partnerships to combat the epidemic. Initiatives embarked upon by the UN shall be considered under this section, as they provide the global vision guiding actions to combat HIV/AIDS.
48The Millennium Development Goals (MDGs), adopted by the UN in 2000, are benchmarks set to measure progress towards the vision of the Millennium Declaration. The eight goals identified to address hunger, gender inequality, child mortality, HIV/AIDS, environmental deterioration and lack of education, health care and clean water seek to promote human well being including dignity, freedom and equality of all people. The MDGS set targets and timelines that should be met by member countries to achieve the goals. HIV/AIDS was identified as a major development challenge and therefore a specific goal to halt the spread of HIV/AIDS by 2015 and to reverse the spread of the pandemic was set. The soaring epidemic has had an impact on the achievement of the other goals as it affects demographic and development trends, including the eradication of poverty, promotion of gender equality, reduction of child mortality and the improvement of maternal health. The United Nations has been collaborating with African countries in various initiatives aimed at scaling up responses to the challenges of the epidemic to meet the targets of the MDGs.
49One of the most important tools in the fight against AIDS is the Global Fund to Fight AIDS, Tuberculosis and Malaria, set up in 2002, following the United Nations General Assembly Special Session on HIV/AIDS. The Fund responds to the pandemic by providing financial resources to affected countries and supporting programs of the most vulnerable people. Sixty per cent of the initial financing from the Fund is for Africa. While the Fund focuses on countries with the greatest present disease burden, it also provides resources to countries at risk in future. Most of the funds have been directed at scaling up the treatment and the provision of Voluntary Counseling Services (VCT). The Global Fund has increased funding for AIDS by committing $1.5 billion and disbursing $131 million so far14.
50In recognition of the high prevalence of HIV/AIDS among women and girls, and the few initiatives on the ground to reduce their high risk, the UN Secretary General, Koffi Annan, in January 2003 established a Task Force on HIV/AIDS, Women and Girls. Five key areas symptomic of the unequal gender relations fueling HIV/AIDS were identified for urgent action by the UN and its partners including national governments, development assistance providers and civil society. The areas are: HIV infection among girls and young women; violence against women and girls; property inheritance rights; the burden of care; and access to HIV/AIDS care and treatment. The activities of the various UN agencies have complimented the UN commitment to fight the pandemic through alliances at various levels. The joint UN Program on HIV/AIDS (UNAIDS), incorporating UNICEF, UNDP, UNFPA, UNDCP, ILO, UNESCO, WHO, WFP and the World Bank, has played a major role in the fight against HIV/AIDS. UNAIDS has been the lead advocate for global action in preventing the spread of HIV; providing care and support for those infected and affected by the disease; reducing the vulnerabilities of individuals and communities to HIV/AIDS; and easing the socioeconomic and human impact of the epidemic. Activities have entailed monitoring, analysing and dissemination of strategic information on the pandemic and global responses to it; encouraging «best practices», that is improved strategies and approaches; building commitment and support among partners; and mobilizing resources for HIV/AIDS programs.
51In assessing the global efforts to fight the epidemic, UNAIDS called for scaled up responses, as the current ones are insufficient to meet the goals set by the UN. Significant progress has been noted in some areas and little progress in others in the past year. Of particular note, national HIV/AIDS strategies and bodies coordinating responses are in place in many countries. Public awareness through various platforms has increased in a large number of countries and funding for programs has increased substantially. However, slow progress has been noted in areas that are critical to sustainable development and human security. Few countries have put in place national policies providing essential support to children orphaned or made vulnerable by HIV/AIDS. In addition, in Sub-Saharan Africa, only 50 000 people were estimated to have access to anti-retroviral treatment at the end of 2002, or about 1% of all the people in need. Anti-discrimination legislation to protect people living with HIV/AIDS has been adopted in only half of the countries in Sub-Saharan Africa15.
52In the years to come, Sub-Saharan Africa is far more certain to experience further demographic changes that would continue to impact negatively on development trends. The epidemic is decimating human capital and institutions, perpetuating intergenerational poverty and inequality, and threatening the security of populations and countries. In this regard, it has become one of the most serious challenges facing African countries. An examination of the impacts of HIV/AIDS in this paper, though not exhaustive, illustrates the huge strain that the epidemic has on individuals, households and governments. This does not necessarily blight prospects for sustainable development and human security on the continent. The cases of Uganda and Senegal have shown that with the appropriate responses, the trend of the epidemic can be reversed or maintained at a very low level.
53Though significant progress has been made in bringing the fight against HIV/AIDS to the forefront of development efforts in Africa, there is still a lot of ground to cover in terms of taking a balanced focus on the various challenges presented by the epidemic. Little attention has thus far been directed on somewhat 'non-conventional' issues to the discourse of HIV/AIDS. Further research on the impact of HIV/AIDS on human security focusing on the implications of the problem of orphans is critical to sustaining human development in Africa. Concrete data to support the general assumptions in the area is imperative to the generation of the much needed political will and commitment to stem the epidemic.
ACRONYMS
54GDP — Gross Domestic Product
55HIV/AIDS — Human Immunodeficiency Virus / Acquired Immunity
56ILO — International Labour Organization
57MDGs — Millennium Development Goals
58SADC — Southern Africa Development Community
59STIs — Sexually Transmitted Infections
60UN — United Nations
61UNAIDS — Joint United Nations AIDS Program
62UNCHR — United Nations Commission for human Rights
63UNDCP — United Nations International Drug Control Program
64UNDP — United Nations Development Program
65UNICEF — United Nations Children’s Fund
66UNESCO — United Nations Educational and Scientific Organization
67UNFPA — United Nations Population Fund
68US — United States of America
69VCT — Voluntary Counselling and Testing
70WHO — World Health Organization
Notes
1 UNFPE State of the World Population Report, 2002 p. 43.
2 Ibid.
3 UNFPA State of the World Report, 2003.
4 UNAIDS, Geographical area Senegal (http://www.unaids.org).
5 UNAIDS, Geographical area Senegal (http://www.unaids.org).
6 UNFPA, State of the World Population 2003.
7 Matinhure, 2003 Paper on demographic impact of AIDS in Zimbabwe.
8 UN Population Division, World Population Prospects 2002 p. 134.
9 Ledec and Goodland 1998, in DuBose
10 UNAIDS, Fact Sheet 2002, Sub-Saharan Africa (http://www.unaids.org).
11 ILO Press release, 11 July 2002.
12 UNAIDS Fact Sheet 2002 AIDS and Security (http://www.unaids.org)
13 Human Development Report 1994
14 Global Fund to Fight AIDS, Tuberculosis and Malaria, Press release 22 September, 2003.
15 UNAIDS, Implementing the Declaration of Commitment on HIV/AIDS, press Release, September 2003.
List of illustrations
 | |
|---|---|
| URL | http://cea.revues.org/docannexe/image/1562/img-1.png |
| File | image/png, 86k |
 | |
| URL | http://cea.revues.org/docannexe/image/1562/img-2.png |
| File | image/png, 103k |
 | |
| URL | http://cea.revues.org/docannexe/image/1562/img-3.png |
| File | image/png, 194k |
 | |
| URL | http://cea.revues.org/docannexe/image/1562/img-4.png |
| File | image/png, 144k |
 | |
| URL | http://cea.revues.org/docannexe/image/1562/img-5.png |
| File | image/png, 109k |
 | |
| URL | http://cea.revues.org/docannexe/image/1562/img-6.png |
| File | image/png, 121k |
 | |
| URL | http://cea.revues.org/docannexe/image/1562/img-7.png |
| File | image/png, 167k |
 | |
| URL | http://cea.revues.org/docannexe/image/1562/img-8.png |
| File | image/png, 81k |
 | |
| URL | http://cea.revues.org/docannexe/image/1562/img-9.png |
| File | image/png, 91k |
References
Bibliographical reference
Victor Angelo, « HIV/AIDS, Population and Sustainable Development », Cadernos de Estudos Africanos, 4 | 2003, 99-120.
Electronic reference
Victor Angelo, « HIV/AIDS, Population and Sustainable Development », Cadernos de Estudos Africanos [Online], 4 | 2003, Online since 15 June 2014, connection on 01 January 2015. URL : http://cea.revues.org/1562 ; DOI : 10.4000/cea.1562
Copyright
© Centro de Estudos Africanos do ISCTE - Instituto Universitário de Lisboa
No comments:
Post a Comment